The Asembia Specialty Pharmacy Summit 2026 convened the industry's most consequential voices at a pivotal moment: clinical innovation is at an all-time high, yet the infrastructure meant to deliver it is fracturing under the weight of fragmented pricing, policy volatility, and decades of administrative inertia.
What emerged from the summit were single six interconnected themes reshaping the future of pharmaceutical access. This recap synthesizes those shifts for Pharma, Health Tech, and Pharmacy leaders building strategy in the year ahead.
The Access Realization Gap
In the modern pharmacy landscape, a doctor's signature is no longer a guarantee of treatment; it is merely the first drop in a high-stakes game of Medical Plinko. For patients, the journey from diagnosis to the first dose has become a chaotic descent through a maze of prior authorizations, rebate walls, and clinical rejections.
As we enter 2026, clinical innovation is at an all-time high, yet the infrastructure meant to deliver it is fracturing. According to McKinsey and Syneos Health, 40–50% of new drug launches now underperform expectations, not because the science fails, but because the environment is changing faster than traditional engagement models can adapt.
The Great Repricing
The era of a single, PBM-dominated pricing model is over. In its place, "The Great Repricing" has fragmented the market into three distinct economies that are increasingly competing for the same products and patients.
With specialty drug spend climbing from 38% in 2014 to 56% of total pharma spend in 2024, and global discounts growing at a 13.3% CAGR, the gross-to-net bubble is no longer theoretical; it is a structural crisis.
The $10 Paradox
The industry has long touted "Price Transparency," but for patients, it has proven to be a mirage. Sticker shock occurs in two phases: the informational shock before treatment, and the harmful shock that arrives via a bill weeks later.
A patient using AI tools to estimate the cost of a specialty infusion might receive an estimate based on public list prices; in reality, their actual out-of-pocket cost after insurance and assistance programs could be a fraction of that.
Surfacing real-time benefit information at the point of prescribing has been shown to reduce first-fill abandonment by 50% to 70%. The goal is no longer transparency; it is Cost Certainty.
The Fax Machine Autopsy
Artificial Intelligence in 2026 is moving past generative hype and into operational Reasoning. In a landmark case study between Mandolin and Amber Specialty Pharmacy, AI Agents didn't just move data; they interpreted it.
Pharma's Guerrilla War
For decades, Pharmacy Benefit Managers held the cards by aggregating demand and controlling the centralized purchasing gate. However, the lack of growth in traditional channels for GLP-1s has forced a strategic pivot. Currently, only 19% of large employers cover GLP-1 weight-loss medications, largely due to PBM-enforced access hurdles.
In response, manufacturers are bypassing the middlemen through Direct-to-Employer (DTE) platforms like Eli Lilly's Employer Connect. By connecting employers directly to telehealth and pharmacy networks, Pharma is reclaiming three critical assets:
- The Data: Reclaiming utilization and adherence data previously guarded by PBMs.
- The Rules: Establishing consistent clinical guidelines and transparent pricing without spread pricing interference.
- The Relationship: Moving the conversation from rebate maximization to measurable health outcomes.
While this risks PBM retaliation against other brands in a manufacturer's portfolio, the shift toward owning the marketplace ecosystem appears irreversible.
The Innovation Brain Drain
While policies like the IRA aim to lower costs, they are triggering a silent exodus of innovation. Market access leaders have shifted from "monitoring" policy to managing "execution risk."
This isn't just about pricing; it is about "Pipeline Herding." Manufacturers are fleeing niches with heavy Medicare footprints in favor of commercial or rare disease markets where the policy floor is more stable.
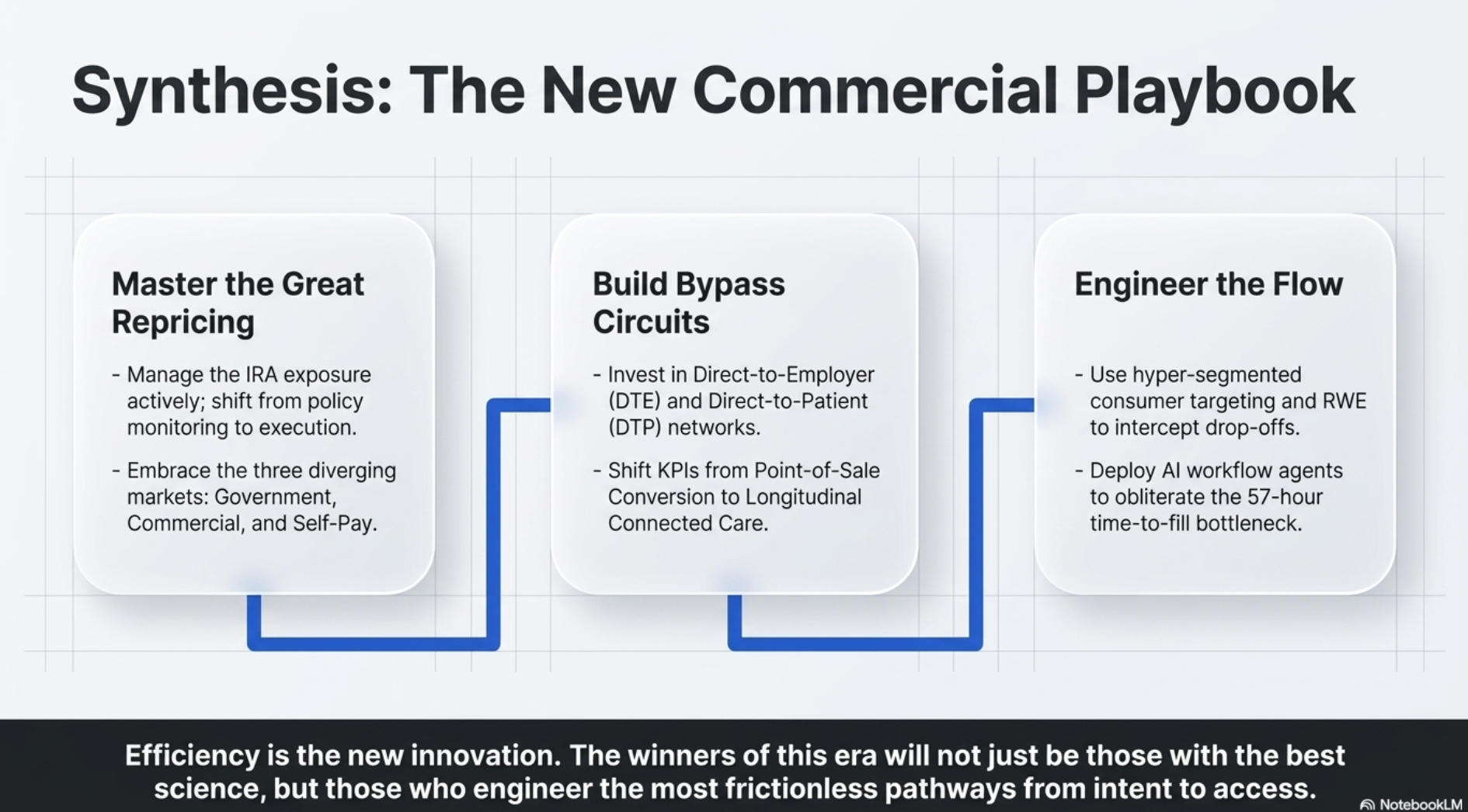
— Asembia 2026 Summit · New Commercial Playbook Synthesis
Conclusion | From Transactions to Persistence
The future of pharmacy is moving from static paths to dynamic flows, transitioning from a transactional model where success is measured by the first script to a longitudinal model centered on Persistence.
As we navigate this brave new world of $3 million gene therapies, AI-driven intake automation, and direct-to-employer marketplaces, the fundamental KPI has changed. The question is no longer "Can we get the drug to the patient?" but "Can we keep the patient on the therapy for the long term?"
In this landscape, the final question remains: In an era of automated care and hyper-stratified pricing, will the human relationship remain at the center of pharmacy — or will we all simply become players in a high-stakes game of Medical Plinko?
About E.fi
E.fi (E-fi) is a strategy and execution firm for visionary leaders solving complex challenges in Pharma, Health Tech, and Government. We help leaders solve the "How do we get there?" problem and get scalable results, faster.
Meet with Us →Disclaimer: This recap is based on conference proceedings and leveraged NotebookLM for synthesis. Provided for general informational purposes only and does not constitute legal, regulatory, financial, or professional advice. Not a substitute for independent evaluation by qualified professionals.